

Fetal Malpresentation and Malposition: Diagnosis and Management
Fetal malpresentation and malposition are significant concerns in obstetric care, as they directly impact the method and safety of childbirth. While the ideal situation for birth involves a fetus in a head-down (vertex) position, facing the mother’s back, this is not always the case. Fetal malpresentation occurs when the part of the fetus closest to the pelvic inlet is not the vertex of the fetal head. Fetal malposition refers to a situation where the fetus is in a vertex presentation, but the fetal occiput (back of the head) is not oriented towards the anterior maternal pelvis. These situations may complicate labor and require careful management to reduce risks to both the mother and the baby.
Understanding fetal malpresentation and malposition is crucial for healthcare providers to ensure the appropriate diagnosis and management. This article provides a comprehensive overview of what fetal malpresentation and malposition are, their types, risk factors, causes, diagnosis, and management strategies, as well as addressing frequently asked questions.
What is Fetal Malpresentation?
Fetal malpresentation refers to any fetal position in which the presenting part entering the birth canal is not the fetal head. Ideally, the baby’s head should be the first to enter the pelvic inlet during labor. This head-first position is called “vertex presentation.” When the baby is not in this position, complications can arise, including a difficult vaginal delivery or the need for a cesarean section.
Types of Fetal Malpresentation
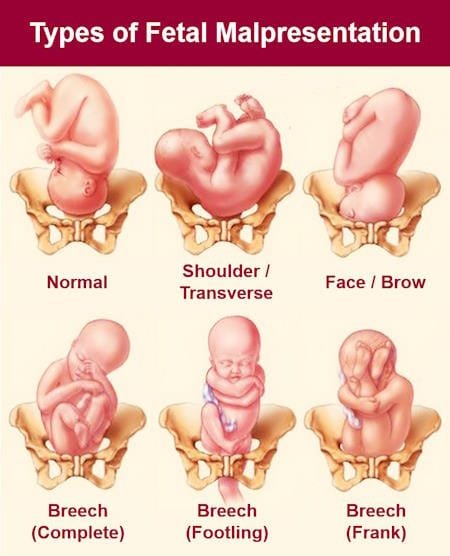
The following are the primary types of fetal malpresentation:
- Breech Presentation: The most common type of malpresentation, in which the baby’s buttocks or feet are positioned to enter the birth canal first. Breech presentations are further categorized into:
- Frank Breech: The baby’s hips are flexed, and legs are extended straight over the body.
- Complete Breech: The baby’s hips and knees are both flexed, with feet and buttocks presenting together.
- Footling Breech: At least one leg is extended, with a foot or both feet entering the birth canal first.
- Face Presentation: The baby is head-first, but the neck is extended, causing the face to present instead of the top of the head.
- Transverse Lie: The baby is lying horizontally in the uterus, with the shoulder, arm, or back over the cervix.
- Oblique Lie: The baby is positioned diagonally, with no part specifically presenting at the cervix.
- Cord Presentation: The umbilical cord is between the baby and the cervix, posing a risk for cord prolapse during labor.
Fetal Malposition
In contrast to malpresentation, fetal malposition refers to the position of a baby that is in vertex (head-down) presentation but with the occiput (back of the head) oriented incorrectly within the maternal pelvis. Optimal positioning involves the occiput facing anteriorly (towards the mother’s front), but in malposition, the occiput faces posteriorly (towards the mother’s back) or laterally (to the side).
The common types of fetal malposition include:
- Occiput Posterior (OP): The baby’s occiput faces the back of the mother’s pelvis, which can lead to prolonged labor and increased discomfort.
- Occiput Transverse (OT): The baby’s occiput is aligned with the mother’s transverse (side) pelvis. This often occurs early in labor, and the fetus may spontaneously rotate to the anterior position as labor progresses.
Causes of Fetal Malpresentation and Malposition
Several factors can contribute to fetal malpresentation and malposition, though in many cases, no definitive cause is identified. Potential causes and risk factors include:
- Placenta Previa: A low-lying placenta can prevent the baby from settling into a head-down position.
- Excessive or Insufficient Amniotic Fluid: Too much or too little amniotic fluid can restrict or allow excessive movement of the fetus, leading to abnormal positioning.
- Uterine Abnormalities: An abnormally shaped uterus or the presence of fibroids can interfere with the baby’s ability to move into the correct position.
- Multiple Pregnancies: Carrying more than one fetus increases the likelihood of malpresentation, as there is less room for each baby to move into an optimal position.
- Previous Malpresentation: If a woman has experienced fetal malpresentation in a previous pregnancy, she is at a higher risk of recurrence.
- Premature Labor: Babies born prematurely are more likely to be in a breech or other abnormal positions, as they may not have had enough time to rotate into the vertex position.
How Common is Fetal Malpresentation and Malposition?
The incidence of fetal malpresentation varies, with reported rates among deliveries at term indicating that:
- Breech Presentation: This occurs in approximately 3% to 5% of term deliveries.
- Oblique or Transverse Lie and Shoulder Presentation: These conditions are relatively rare, occurring in less than 0.05% of cases.
- Face and Brow Presentations: Both types of presentations are estimated to occur in 0.1% to 0.2% of deliveries.
- Compound Presentation: This also occurs in about 0.1% to 0.2% of cases.
Overall, studies have shown that the incidence of malpresentation is around 2.5%, with breech being the most common type encountered.
Persistent fetal malpositions are reported at varying rates among all deliveries, including:
- Occiput Posterior Position: This occurs in approximately 20% to 30% of fetuses at full cervical dilatation. Among them most will rotate spontaneously and only 5% to 10% will deliver in a persistent Occiput Posterior position.
- Occiput Transverse Position: Upto 50% of fetuses are Occiput Transverse at the onset of the labor. The prevalence falls to 19% to 30% in the second stage of labor and only 3-8% at the time of delivery.
In normal fetal positioning, fetuses in cephalic lie, vertex position, and occiput anterior position are most likely to deliver vaginally. When the fetal head is flexed and the vertex is occiput anterior, the effective diameter of the fetal head is minimized, optimizing the shape of the fetal head to navigate through the maternal pelvis. It is common for vertex-presenting fetuses to be in an occiput transverse position during early labor, but most will spontaneously rotate to the occiput anterior position as labor progresses.
Diagnosis of Fetal Malpresentation and Malposition
Diagnosing fetal malpresentation and malposition typically involves a physical examination and imaging. Your healthcare provider may use the following methods:
- Abdominal Palpation: By feeling the mother’s abdomen, the healthcare provider can estimate the baby’s position.
- Vaginal Examination: During labor, a vaginal exam may reveal which part of the baby is presenting in the birth canal.
- Ultrasound: If the baby’s position is unclear, an ultrasound can confirm the exact presentation and position of the fetus.
Can the Baby’s Position Be Changed?
In some cases, it may be possible to change the baby’s position before labor begins. External cephalic version (ECV) is a common procedure used to turn a breech baby into the vertex position. It is typically performed after 36 weeks of pregnancy.
External Cephalic Version (ECV)
During an ECV, a healthcare provider manually applies pressure to the mother’s abdomen to rotate the baby into a head-down position. While this procedure can be successful, it is not always effective, and some babies may return to the breech position after being turned.
Alternative Methods
Some women may try alternative techniques, such as postural exercises, acupuncture, or moxibustion, to encourage the baby to turn. While evidence for these methods is limited, moxibustion, in particular, has shown some promise when performed before 37 weeks of pregnancy. However, it is always recommended to discuss these options with your healthcare provider before trying them.
Management of Fetal Malpresentation and Malposition
Cesarean Delivery
The majority of babies in breech presentation, or other forms of malpresentation, are delivered by cesarean section, as this is generally considered safer for the baby. Cesarean delivery can help avoid potential complications that may arise from attempting a vaginal delivery when the baby is not in a head-first position.
Vaginal Breech Delivery
In some cases, a vaginal breech delivery may be attempted, particularly if the baby is in the frank breech position, and the hospital has the necessary expertise and equipment. However, vaginal breech delivery carries risks, including the possibility that the baby’s head may become stuck during delivery, leading to a medical emergency.
Managing Occiput Posterior and Occiput Transverse Positions
Babies in occiput posterior or occiput transverse positions can often still be delivered vaginally. However, labor may be longer, and the mother may experience more pain, particularly in the lower back. In many cases, the baby will rotate to the optimal position during labor, but interventions such as manual rotation or the use of forceps may be necessary.
Risks of Fetal Malpresentation and Malposition
Fetal malpresentation and malposition can increase the risk of complications during delivery, including:
- Cord Prolapse: When the umbilical cord enters the birth canal before the baby, it can become compressed, cutting off the baby’s blood supply.
- Prolonged Labor: Malpositioned babies may result in a longer labor, which can increase the risk of complications for both the mother and baby.
- Birth Injuries: Vaginal delivery in cases of malpresentation can result in injuries to the baby, including fractures, dislocations, and nerve damage (e.g., Erb’s palsy).
- Emergency Cesarean Section: Many women who attempt vaginal breech delivery or labor with a malpositioned baby end up needing an emergency cesarean section, which carries a higher risk of complications compared to a planned cesarean.
Will I Have a Malpresentation in Future Pregnancies?
Having experienced a malpresentation or malposition in one pregnancy does increase the risk of it occurring in future pregnancies. However, many women successfully deliver subsequent babies in the vertex position. A healthcare provider can assess risk factors and help develop a delivery plan to minimize the chances of malpresentation in the future.
Conclusion
Fetal malpresentation and malposition are important considerations in the management of pregnancy and labor. Understanding the types, causes, diagnosis, and management of these conditions can help healthcare providers ensure the safest delivery for mothers and their babies. While some situations require surgical intervention, such as cesarean delivery, others may allow for vaginal birth with appropriate monitoring and management. It is essential for expectant mothers to maintain open communication with their healthcare providers and discuss any concerns related to fetal positioning during pregnancy.








